5 TIPS TO TREAT KNEE PAIN IN RUNNERS
 By: Dr. Rachel Jakubowski
By: Dr. Rachel JakubowskiPhysical Therapist
SPECTRUM, Inc
I want to start off by talking about a client I saw a few months ago for knee pain named Ali. Ali is 48 years old and an avid runner. She runs 3-4 miles every other day and enjoys competing in half marathons. Her favorite races are Disney’s Princess and Wine and Dine Half Marathons. She came to me because she had been experiencing dull, achy knee pain that sometimes shoots into the inner part of her knee with running. At first she kept running through her pain but eventually it got so bad she had to completely stop running. She first sought out a massage therapist but was only getting temporary relief. She then tried physical therapy at a corporate clinic and found that she wasn’t getting the quick results she desired because she was rehabbing with four other people. A friend ended up recommending her to Spectrum Physical Therapy. We performed a thorough full body movement screen, identified her specific dysfunctions, and got her back to running 3-4 miles in 4 weeks.
I know a lot of people fit in this category…They don’t know what’s wrong with them. They don’t know what will help. They hope it will just go away with time so they keep running. They tried resting briefly but the pain came back once they started running again.
The goal of this blog is to provide examples on common dysfunctions I see in individuals with knee pain and exercises I typically provide to combat knee pain. I want you running the miles you want without being held back by pain!
By the time I’ve seen most runners they’ve either self-diagnosed or have been told by a physician that they have arthritis, distal IT band syndrome, patellofemoral syndrome (PFPS), etc. It always makes people feel better to have a diagnosis but some of these diagnoses are considered “garbage terms.” For instance, PFPS includes chondromalacia, patellar tendonitis, general anterior knee pain, etc. What I consider to be more important than the medical diagnosis for this condition (the PFPS designation), is the movement diagnosis (hip weakness, tight quads, etc.). Your knee pain just didn’t appear out of thin air. It appeared because of a mechanical problem and to fix the problem you need to figure out the “why” — the movement diagnosis.
5 common dysfunctions and exercises I see in runners with knee pain:
1. Pelvis is out of alignment
2. Poor Hip/Core Stability
3. Restricted Ankle Range of Motion
4. Tibial Bone Rests in External Rotation
5. Knee Valgus Collapse
[For the videos without verbal explanations–look below the video exercise descriptions and reps/sets]
For more information on each of these dysfunctions read below:
1. Pelvis is out of alignment: Postural Restoration Institute (PRI) has found that our body has a tendency to develop a pelvic shift forward on one side because of asymmetrical positioning of our organs. This forward pelvis shift changes the alignment of the femur bone as it sits in the hip joint and can restrict hip range of motion due to this change, becoming a potential problem for active individuals. It also makes us favor one side or our body when we are running which can lead to overuse on one side. This asymmetry trickles down to the knees and the ankles by changing how weight is distributed over different joints in the lower body. When you then add pounding on your joints from running it can place unwanted stress on your knee, hip and ankle that can then turn into pain.
2. Poor Hip/Core Stability: Another common problem for runners is poor core and hip strength/stability. When your hips and core are weak, your knees take on a lot of extra work. There are your six pack abs (rectus abdominis, obliques, back extensors), and then there is your deeper inner core. The deep inner core is extremely important in how your body stabilizes during movement and I find this more of a problem at times then the big six pack ab type muscles. So instead of just adding more sit ups or planks, try diaphragmatic breathing.
If you experience incontinence (urine leakage) during sports or coughing you most likely have a pelvic floor weakness–in these cases you should see a pelvic health specialist.
3. Restricted Ankle Range of Motion: Ankle Dorsiflexion (the amount of available range of motion bringing your foot up to your shin) is extremely important in runners for a few reasons. If you don’t have full range of motion bringing your foot to your shin, then your foot will have a tendency to turn outward—”duck walking.” When your foot significantly turns outward during running, it places a lot of stress not only at the inner side of your knee but also on the muscles/ligaments/tendons at your foot and ankle. This problem is a common cause of achilles tendonapathy, shin splints, and plantar fasciitis as well.

Ankle dorsiflexion
4. Tibial Bone Rests in External Rotation: When looking at lower leg alignment your tibia, or your shin bone, should face straight forward. I see a lot of individuals with shin bones rotated outward. So (like in the picture below), if your knee caps are facing straight forward your feet should generally face forward as well. A slight toe out is okay, but more significant “toeing out” can become an issue. As you can see on the right, the knee caps are facing forward and the foot is pointed out significantly. With this problem, ankle dorsiflexion can be restricted and a lot of pressure is placed on the inner aspect of the knee when walking or running.
Restricted knee joint mobility or tight IT bands can pull the tibia outward.

Sometimes; however, the “toe out” position can be due to a congenital deformity in the hip or tibia which cannot be fixed
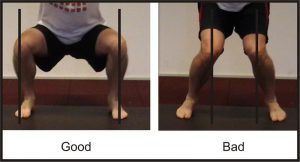
5. Knee Valgus Collapse: Knee Valgus collapse is simple because it ties into hip and ankle problems already addressed. If you notice your knees drop inward when you squat, run or jump this is a huge problem. Poor core/hip stability, poor ankle mobility, pelvis and tibial alignment issues all cause this problem (as seen below in the picture).
Leave a Reply